
Definition
A fracture is a discontinuity in a bone (or cartilage) resulting from mechanical forces that exceed the bones’ ability to withstand them.[1]
A fracture is often written as # in medical shorthand, i.e. the hash symbol, although it is still pronounced as fracture, e.g. “neck of femur fracture”, may be written as “#NOF”.
Most commonly fractures occur in the setting of a normal bone with acute overwhelming force, usually in the setting of trauma. Fractures can also occur, however, in a variety of other settings.
Firstly, the entire skeleton may be weak due to metabolic (e.g. osteoporosis) or less frequently genetic abnormalities (e.g. osteogenesis imperfecta) and thus prone to fractures from forces that would be insufficient to cause fractures in normal bones. These are known as insufficiency fractures.
Secondly, the protracted chronic application of abnormal stresses (e.g. running) can result in the accumulation of microfractures faster than the body can heal, eventually resulting in macroscopic failure. These are termed fatigue fractures.
Together, insufficiency and fatigue fractures are often grouped together as stress fractures.
Thirdly, the bone may have a lesion that focally weakens it (e.g. metastasis, bone cyst, etc). These are known as pathological fractures.
Rarely the term ‘fracture’ is also used for non-osseous/chondral structures (e.g. penile fracture) although if unqualified it is assumed one is referring to a bony fracture.
Although many eponymous fractures exist and the relevant particulars of a fracture will depend on its specific location, generally fractures are described in a consistent manner:
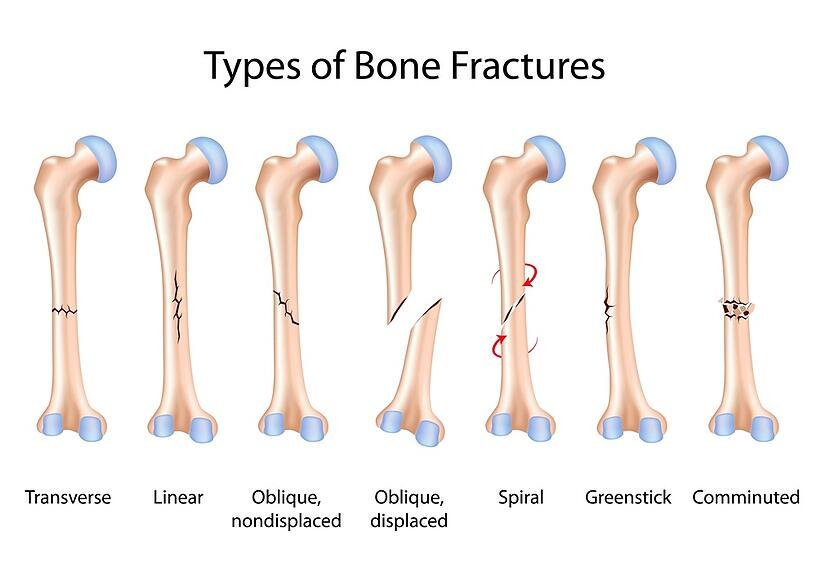
Types of Bone Fracture
Fractures are usually of following types-
- Complete fracture.
- Transverse fracture.
- Oblique fracture.
- Spiral fracture.
- Comminuted fracture.
- Incomplete fracture.
- Green-stick fracture: the cortex breaks, but only on one side
The fracture has many classifications, depending upon the position of the bone fracture, displaced or non-displaced. Complete or incomplete fracture. Transverse or vertical fracture according to the orientation of the fracture. Simple or compound according to the penetration of the skin.
Pathophysiology
The pathophysiological sequence of events that occur following a fracture can be divided into three main phases:
- Inflammatory
- Reparative
- Remodeling
Inflammatory Phase
Immediately at the time of fracture, the space between fracture ends gets filled with blood-forming a hematoma.
· Stops additional bleeding; provides structural and biochemical support for the influx of inflammatory cells, fibroblasts, chondroblast, and the ingrowth of capillaries
This process takes approximately a week, forming a primary callus which is non-mineralized and not readily visible on radiography
Reparative Phase
Over the next few weeks, this primary callus is transformed into a bony callus by the activation of osteoprogenitor cells. These cells lay down woven bone which stabilizes the fracture site.
Remodeling Phase
This phase lasts many months, maybe years, and represents the gradual formation of compact cortical bone with greater biomechanical properties and allows for the reduction of the width of the callus. Remodeling can cause almost perfect healing, however, particularly if the alignment is not perfect, a residual deformity will remain.
Complications
Many of the aforementioned fracture types can also go on to have additional complicating features.
- Acute compartment syndrome is common in a fractured forearm.
- Fat embolism syndrome (a piece of fat that released into the blood vessels causing blockage of blood flow) that is most commonly associated with long bone and pelvic fracture
- Osteomyelitis of bone in response to infection.
- Healing complications: malunion, delayed union, or nonunion.
- Avascular necrosis
- Fracture blisters
- Compound fracture: extending through the skin
- Joint involvement: intracapsular; articular; dislocation. [2]
Role of Physiotherapy

The physiotherapist’s role is to identify the cause of the problem and to select the appropriate procedure to alleviate or eliminate the cause of the loss of movement. Examples of early treatment include
- A physical therapist may instruct the client how to walk with an assistive device, like a cane or crutches. This includes how to use the device to walk up and down stairs or to get into and out of a car. Learning a new skill takes practice, so be sure to allow client practice using your device while they are with you.
- After a lower extremity fracture there may limit the amount of weight client can put on the leg. Help the client understand weight bearing restrictions and teach how to move about while still maintaining these restrictions.
- If the fracture is in the arm, you as the physical therapist may teach you how to apply and remove the sling
Doing an assessment for the patient is necessary also doing The problem-oriented medical record (POMR) system ( is based on a data collection system that incorporates the acronym SOAP:
- Subjective – any information given to you by the patient: allergies, past medical history, past surgical history, family history, social history (living arrangements, social conditions, employment, medication), review of systems .
- Objective – all information obtained through observation or testing, e.g. range of joint movement, muscle strength .
- Analysis – a listing of problems based on what you know from a review of subjective and objective data.
- Plan – this refers to the plan of treatment).
Also By Using specific exercises, the aim is to reduce any swelling, regain full muscle power and joint movement, and to bring back full function. The treatment will depend very much on the problems identified during your initial assessment, but may include a mixture of the following:
- Soft tissue massage, particularly to manage Edema and swelling
- Scar management if the patient had surgery to fix the fracture
- Ice therapy
- Stretching exercises to regain joint range of movement
- Joint manual therapy and mobilizations to assist in regaining joint mobility
- Structured and progressive strengthening regime
- Balance and control work and gait (walking) re-education where appropriate
- Taping to support the injured area/help with swelling management
- Return to sport preparatory work and advice where required.[3]
STUDIES
Study 1
International Journal of Science and Research (IJSR)
Case Study – Post Operative Rehabilitation of
Fracture of Distal End of Radius
Abstract: Introduction: Fracture of the distal end radius constitutes one of the most common skeletal injuries treated by the orthopedic surgeon. Wide arrays of techniques have been described including closed reduction, percutaneous fixation and open methods of reduction, and stabilization. Open reduction and internal fixation of distal radial fractures with an angular stable locking plate applied to the volar surface has gained vast popularity recently.
Methodology: This case study was conducted on Mr D.S.Dahiya during the first week of November 2016 to last week of february 2016 in total 4months. The patient came to me with a post operative closed fracture distal end of radius the process of the therapy started with initial kinesiological examination followed by 4 months long therapy session and a final kinesiological examination.
Therapy Process: The patient got a treatment with passive interventions to improve circulation and prevent immobilization adhesion formation. These treatments included application of an ice pack to reduce edema followed by application of a wax bath on the affected wrist. Gentle range of motion mobilizations were then introduced that could only be performed in flexion and extension to the patient’s pain tolerance.
Final Kinesiological Examination Conclusion: Daily wrist and hand ROM was measured prior and post treatment. The final kinesiological was performed on 28th Feb 2017 and showed the patient’s improvement to the therapy applied. The patient came for physiotherapy for lack of muscular strength and limited mobility in the affected area. The final examination shows patients improvement in muscular strength, mobility and muscle shortness after 4 months of therapy.
Conclusion: During the 4 months of Physiotherapy sessions, we had with the patient, we both could see the improvement from day 1 until our last session together. He improved greatly during the course of 4months the rapid improvement came after functional training with mobilizations and Sustained Stretching of wrist flexors with the pillow underneath.[4]Click here to Read full article
Study 2
University of North Dakota
UND Scholarly Commons
Physical Therapy Treatment for a Patient with a Hip
Fracture and Cognitive Impairments: A Case
Report
Abstract • The patient in this case report was a 78 year-old female who sustained a femoral neck fracture after a fall. The fracture was repaired surgically with a hip hemiarthroplasty procedure. The patient received physical therapy interventions over the course of seven weeks at a transitional care unit. • Physical therapy interventions for this patient included: • Gait Training • Patient Education • Transfer Training • Strengthening Exercise •Balance Activities • The patient had co morbidities that increased her risk of falling such as osteoporosis, history of falls, and cognitive impairment. Cognitive impairment can affect the quality of care, patient rapport, and treatment plan. Physical therapy interventions were modified for this patient using frequent tactile cueing during exercise. This ensured proper form and optimal results. • The patienfs goals were to return to her prior level of function. In order to return to her home at a memory care unil She had to be able to perform all activities of daily living and transfers independently. • Through physical therapy interventions, the patient was able to meet all of her goals, increase strength and range of motion, and returner to her memory care unit apartment. [5]Click here to Read full article
Study 3
Abstract : A Case- Study of physiotherapy treatment of a patient who has experienced ankle fracture in his right leg.
Goal: The main objective of this thesis is the discuss all information related to ankle fracture along with the rehabilitation plan to recover the ankle fracture, which will be discussed in the theoretical and practical section of this thesis. The theoretical part highlights the historical information, lower extremities anatomy, biomechanics and kinesiology of the ankle joint, different injury types and the rehabilitation plan. The clinical picture and the etiology of this fracture along with specific tests for ankle fractures will also be discussed. The practical part presents a male patient case study that recently experienced ankle fracture.
Methods: The rehabilitation process of this patient majorly focused on the use of isometric exercises, soft tissue techniques, sensorimotoric exercises and muscle stretching and strengthening. It included a total of 8 therapy sessions where each session lasted for 30 minutes to 60 minutes along with two additional sessions where the initial and final kinesiologic examinations were performed. Results: During these two weeks of rehabilitation, the patient demonstrated considerable improvement in his ankle condition and had increased the active and passive range of motion in his broken ankle. He also reported a decrease in the pain intensity and was able to walk independently and smoothly.
Conclusion: Based on the initial and final kinesiologic examination, it was evident that the patient demonstrated a high level of satisfaction with the improvement in his ankle condition. The rehabilitation therapies aided him in being fully active and independent.[6] Click here to Read full article
References–
[1] RadioPedia https://radiopaedia.org/articles/fracture-1
[2] Wikipedia https://en.wikipedia.org/wiki/Bone_fracture
[3] Physio Pedia https://www.physio-pedia.com/Fracture
